Demographic Profiling
The identification of individuals who may potentially be at risk for exposure to tuberculosis is dependent upon the recognition of the current socio-spatial distribution of the disease, and the members of ethnic communities, age classes and residents of particular areas that it affects disproportionately. Indexing common socio-economic and locational variables that characterize groups of active TB patients is critical to the process of identifying individuals who have the greatest expected risk of infection by Tuberculosis in the near future. Profiling was an important step as it allowed us to acquire a more complete, comprehensive understanding of the socio-geographic dimensions of tuberculosis in the Greater Vancouver area, and it facilitated a means by which to visualise the non-statistical elements of the dataset.
The Lung Association of Canada outlines risk factors and behaviours that may act alone or in concert to increase the degree of individuals' exposure to TB, including:
i. Close and prolonged contact with persons with active TB
ii. Immigration from areas around the world where TB is common and/or infection rate is high
iii. History of immune suppression therapy, or an inherently weak immune system that may reduce one's ability to fight infection
iv. Alcoholism
v. Intravenous drug use
vi. Homelessness and/or residence in shelters or hostels
vii. Employment at, or residence in, long-term care facilities
viii. Employment or time spent at hospitals and/or correctional centres
ix. The elderly, especially those living at times of TB epidemics
Other variables identified in the literature as increasing the risk of individuals to tuberculosis exposure included:
i. Exposure to HIV/AIDS, or incidence thereof
ii. Years of immigration, indicating whether persons coming from certain countries were exposed to epidemics
iii. Age - both young children and the elderly have weaker immune systems, meaning that they are more prone to infection by various diseases, including tuberculosis.
Profiling began by looking for overall trends in the GVRD dataset with respect
to age class (0-25, 23-50, 50+), ethnicity, birthplace (Canadian born vs. foreign
born), predisposing conditions with particular focus on HIV/AIDS and diabetes,
areas of residence with particular emphasis on the Downtown Eastside, and gender.
The dataset was then repeatedly queried by ethnicity for frequencies of the
above-mentioned variables amongst active-TB patients. Profiling was conducted
on the base of ethnicity because significant occurrence of specific factors
often appeared to affect particular ethnic groups. To illustrate this point,
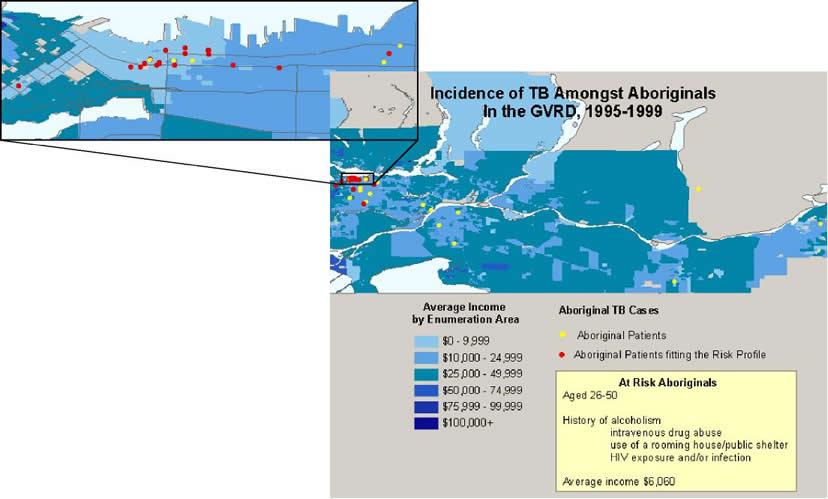
HIV positivity and full-blown AIDS were prominent amongst 25 percent of Aboriginal
individuals with active TB, whereas it was far less important of a risk factor
(if a risk factor at all) amongst the other ethnicities.
Proportionally high frequencies of risks within ethnic groups were isolated and assumed to predispose persons of that ethnicity to greater risk of TB infection. Once several factors were identified as characterizing the demography of tuberculosis for a particular ethnicity, we began to search for shared variables and the range of ages in which they were prevalent. Un-diagnosed individuals of respective ethnic communities are thus considered to be "at risk" if they meet all the necessary and any of the secondary conditions that characterize the active-TB patients of corresponding ethnic origin. When certain behaviours and demographic variables repeatedly typify active-TB patients belonging to certain ethnic groups, and surface much less frequently amongst diagnosed patients belonging to other ethnic groups, the assumption arises that individuals engaging in the same behaviours or migratory histories (for example, foreign born persons immigrating from country x within the same five-year time frame, shortly after a TB outbreak in the source country) that presently un-diagnosed members of that ethnic community sharing similar characteristics are at greater risk of developing or contracting active TB than other members of the same ethnic origin.
Via this process, five broad "At Risk" profile categories were
developed.
1. An Aboriginal living in the DTES aged 31-50. S/he is generally an alcoholic, and IV drug abuser, and/or HIV positive. Also, there is a good chance of having used a rooming house within the past year.
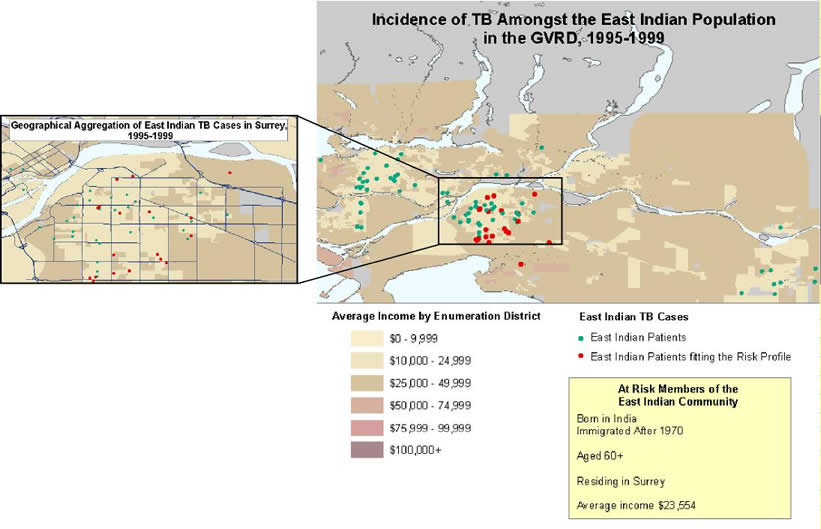
2. A member of the East Indian community born outside of Canada (in India) who is over the age of 60 and immigrated to Canada after 1970. The individual currently resides in Surrey.
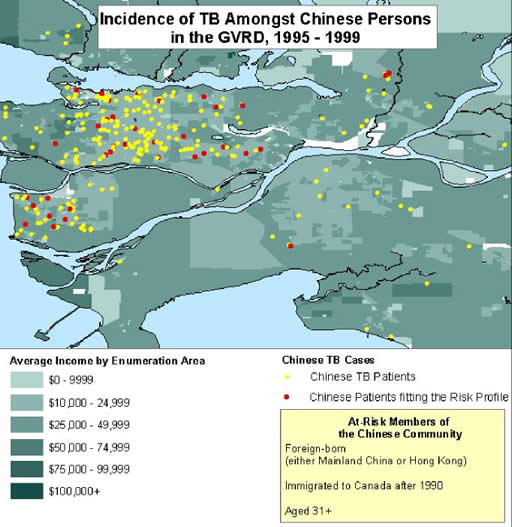
3. Foreign-Born Chinese (either Mainland China or Honk Kong) who immigrated here after 1990, and are of 31 years of age or older.
4. A Canadian-born white male living in Vancouver who has a high chance of being
an alcoholic, IV drug abuser, or HIV-positive. Ages tend to be fairly spread
out but a little higher between the ages of 31-50 and 71-80.

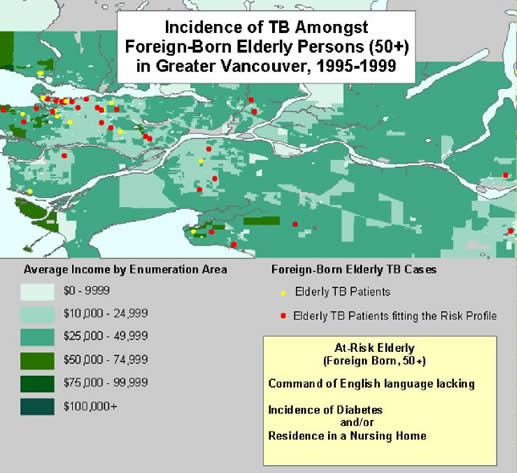
5. An elderly person (50+) who was not born in Canada and does not possess a
competent command of English. The person may be living in a nursing home and
may have diabetes.
Methodology
& Analysis
Visualization | Demographic Profiling | MCE
| Spatial Statistics
Home
| Introduction | Background
Objectives | Data
| Analysis | Error | Conclusions
Links | References
| Contact