Past Projects
GLOBAL HEALTH
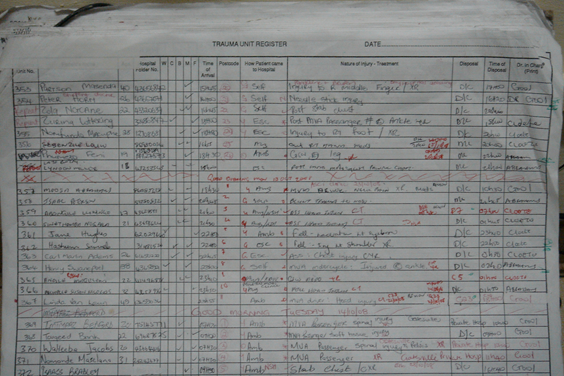
My interest in global health began in Cape Town, South Africa, where I worked with Dr. Morad Hameed (Stanford University) and graduate students, we developed an injury surveillance system to document severe injuries as patients are admitted to hospital. The surveillance system was designed to improve patient care as well as to target prevention efforts. Human resources are scarce in Low and Middle Income Countries (LMIC). To that end, our injury surveillance was focused on parsimonious data collection that can be deployed in very low resource settings.
Dr. Leah Rosenkrantz continued this work on trauma surveillance during her PhD.



MATERNAL HEALTH
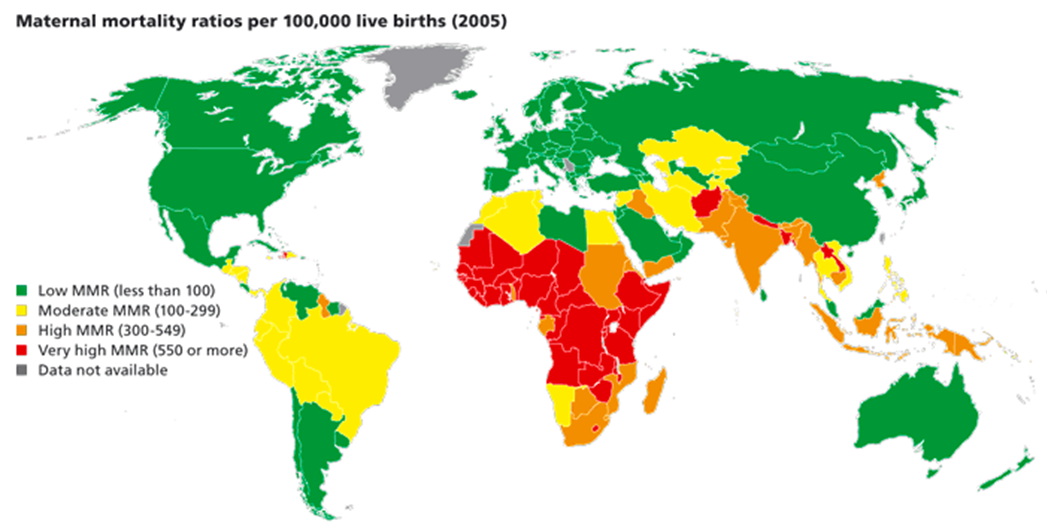
Maternal health is a pressing issue worldwide. I have joined a UBC team focused on reducing pre-eclampsia in low and middle income countries. I introduced the concept of maternal resilience to highlight areas where maternal outcomes are positive - despite poor environmental conditions. My former PhD student, Tatenda Makanaga, and I worked on a project to develop an index of maternal resilience in LMIC - as well as in Canada where aboriginal infant mortality is ten times higher than in the general population. We were uniquely focused on environmental correlates with maternal health including overcrowding, access to running water and latrines, and access to health services. Dr. Makanga has continued to work on these issues in Zimbabwe and the UK.

MULTIPLE SCLEROSIS
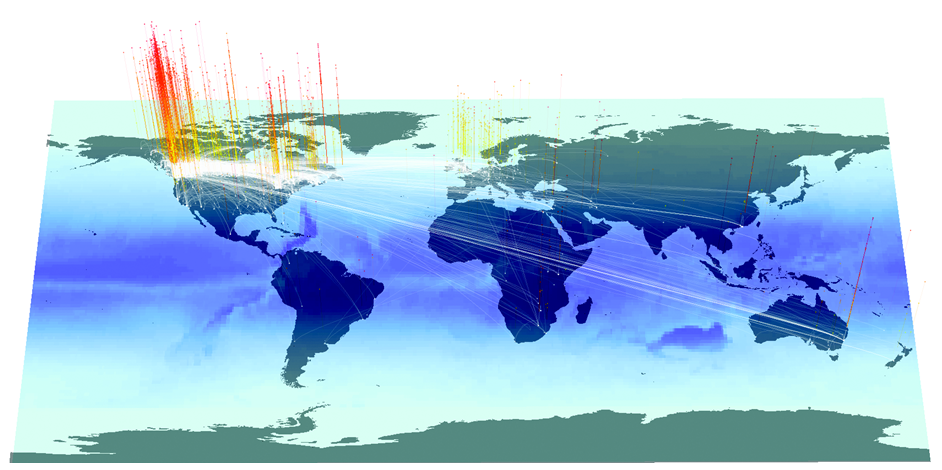
Multiple sclerosis (MS) is a chronic, degenerative disease of the central nervous system. The exact cause of MS is not yet understood. Multiple risk factors may be involved including interactions between susceptibility genes and environmental factors. Several clinical and epidemiological studies support the hypothesis that vitamin D levels – perhaps mediated by ultraviolet B (UVB) exposure – are able to modulate disease processes in MS. Over the past 50 years, empirical data has indicated that increased latitude is linked to greater prevalence of MS. However, direct causation has not been proven, especially in the light of confounding factors – such as multiple moves over a lifetime. Working with Dr. Helen Tremlett at UBC and a former PhD student (Ofer Amram), we developed a protocol to calculate total UVB exposure over the lifetime of patients. We were able to use detailed life histories of 4000 patients combined with TOMS data from NOAA to develop this methodology. This protocol applies geographical concepts to better understand the etiology of a prevalent disease.
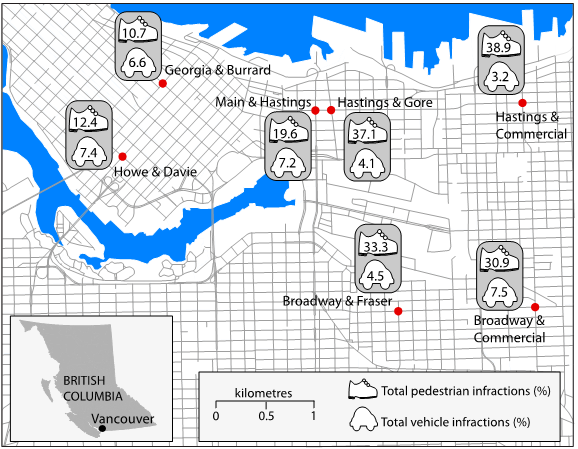
INJURY AND THE BUILT ENVIRONMENT
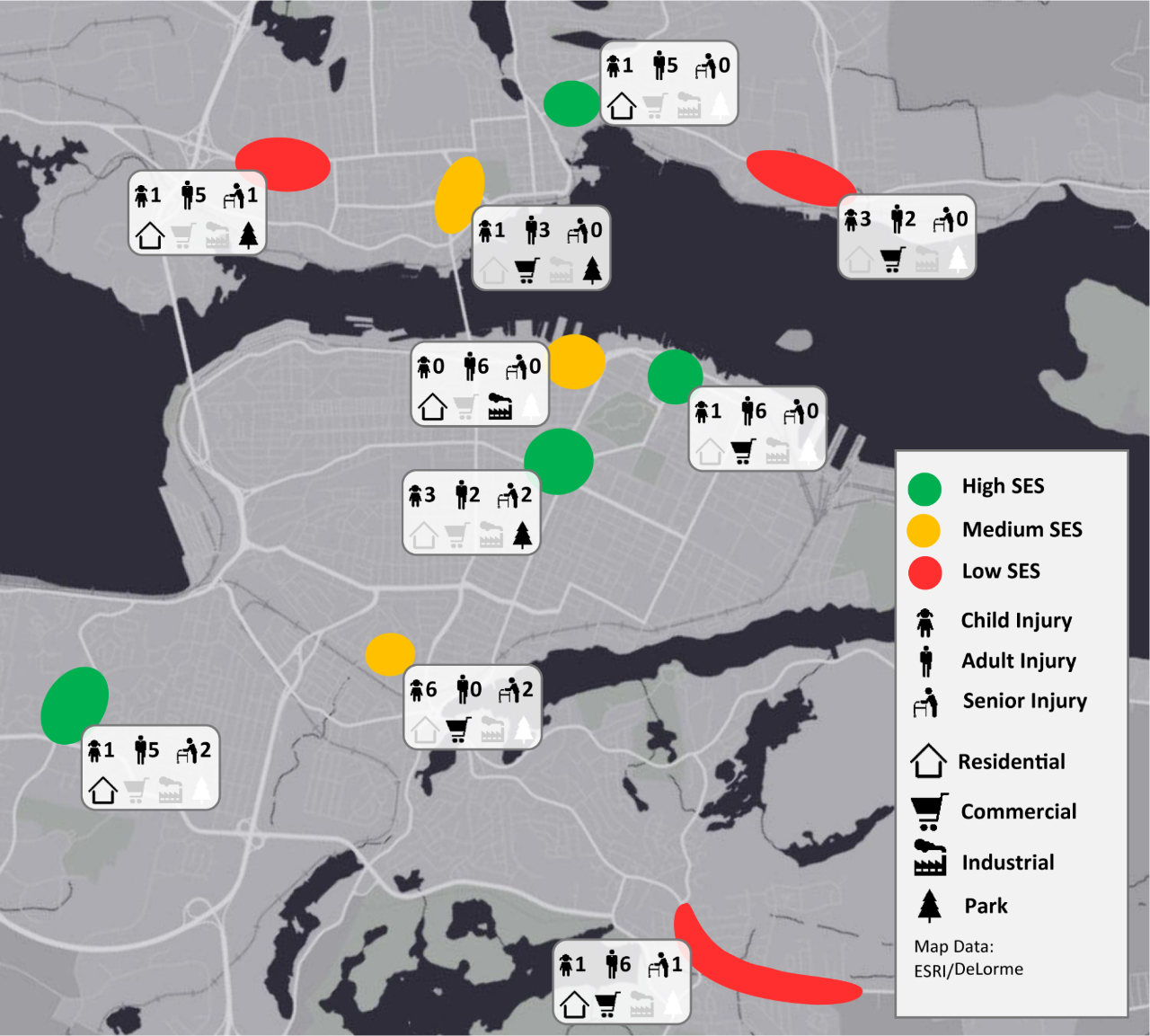
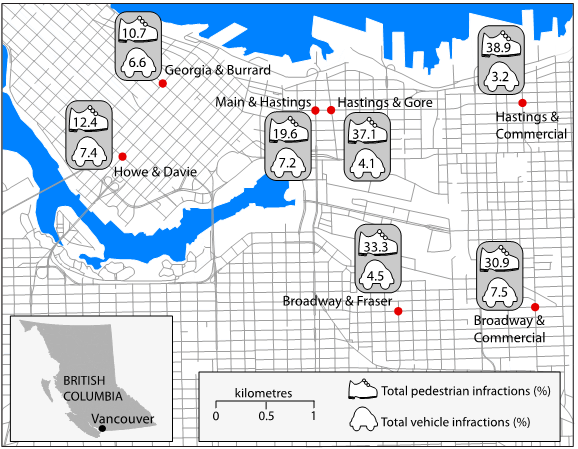
The relationship between injury and the built environment has historically been poorly understood. I have conducted several studies that articulate clear links between pedestrian injury and the environment. I developed a methodology that allows us to conduct environmental scans of urban injury hotspots. Our team then conducted environmental scans at each hotspot to determine environmental correlates with injuries. We have now integrated this method into several new studies, including those on Runnability and Overdose Geography.

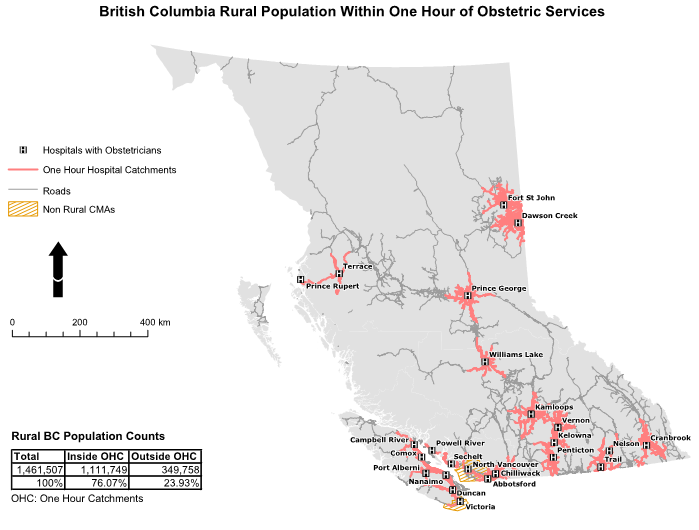
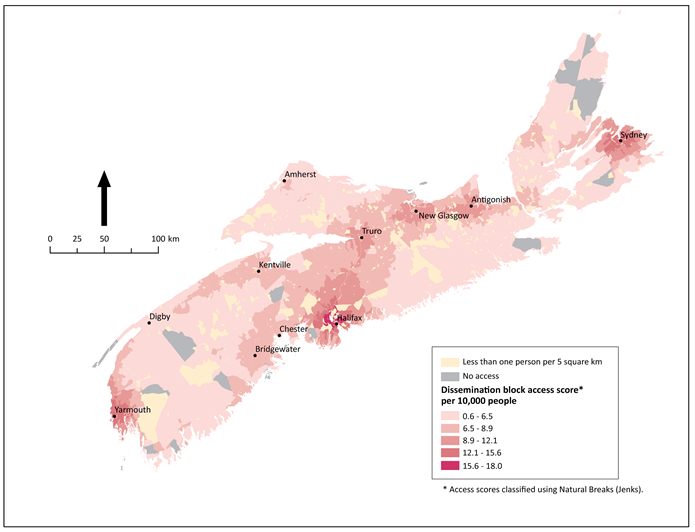
ACCESS TO HEALTH SERVICES
A final cornerstone of my research has focused on access to health services. It is an axiom of health research that access increases positive health outcomes. However, access (both spatial and socially enabled) is geographically disparate. In my lab, we have developed methods to measure potential spatial access to a range of health services. We link travel time access to population catchments to determine areas where services need to be intensified and use the results to contribute to evidence-based decision-making.